ARUSHI KUMARI
GENERAL MEDICINE DEPARTMENT
ONLINE BLENDED BIMONTHLY ASSIGNMENT
NAME : ARUSHI KUMARI
SEMESTER : VIII
ROLL NO : 151
Question 1. What is myelopathy hand ?
Answer. It is a characteristic dysfunction of the hand observed in various cervical spinal disorders when there is involvement of the spinal cord
- There is loss of power of adduction and extension of the ulnar two or three fingers and inability to grip and release rapidly with these fingers.
- These changes have been termed "myelopathy hand" and appear to be due to pyramidal tract involvement.
- The characteristic nature of the signs permit the distinction between myelopathy and changes due to nerve root or peripheral nerve disorder.

Fig : Cevical Spondylotic Myelopathy
Question2. What is Finger Escape ?
Answer. Wartenberg's sign is a neurological sign consisting of involuntary abduction of the fifth (little) finger, caused by unopposed action of the Extensor Digiti Minimi.
- This commonly results from weakness of some of the ulnar nerve innervated intrinsic hand muscles-in particular the Palmar interosseous muscle to the little finger- caused by damage to their nerve supply (denervation).
- It is seen in Cervical Myelopathy most commonly due to mechanical compression of the spinal cord in the neck as occurs in spondylotic cervical canal stenosis but also seen in other spinal cord disease including post- traumatic tetraplegia. This finding of weak finger addiction in cervical myelopathy is also called the " finger escape sign .

Fig : Digitii Quinto Sign
Question 3. What is Hoffman's Reflex ?
Answer. Hoffmann's reflex is a neurological examination finding elicited by a reflex test which can help verify the presence or absence of issues arising from the corticospinal tract .
- It is named after neurologist Johann Hoffmann.
- Usually considered a pathological reflex in a clinical setting, the Hoffmann's reflex has also been used as a measure of spinal reflex processing (adaptation) in response to exercise training .
Procedure :
- The Hoffmann's reflex test itself involves loosely holding the middle finger and flicking the fingernail downward, allowing the middle finger to flick upward reflexively.
- A positive response is seen when there is flexion and adduction of the thumb on the same hand .
Interpretation :
- A positive Hoffmann’s reflex and finger jerks suggest hypertonia, but can occur in healthy individuals, and are not useful signs in isolation.
- In cerebellar diseases, the reflexes may be pendular and muscle contraction and relaxation tend to be slow, but these are not sensitive or specific to cerebellar signs.


Figure : Evoking a Hoffman reflex
Question 1. What can be the cause of her condition ?
Answer . According to MRI Cortical vein thrombosis might be the cause of her seizures .
Question 2 . What are the risk factor for cortical vein thrombosis ?
Answer. The various risk factors for cortical vein thrombosis in infants and children are:
꘎ Sickle cell anemia
܁꘎ Chronic Hemolytic Anemia
܁꘎ Congenital or acquired heart disease
܁꘎ Iron deficiency anemia
܁꘎ Dehydration
܁꘎ Infections
܁꘎ Head injury
܁꘎ For Newborn ,from the mother who had H/o infection or H/o infertility
The various risk factor for cortical vein thrombosis in adults are :
܁꘎ Pregnancy and first few weeks after pregnancy
܁꘎ Disorder of blood clotting , e.g., Antiphospholipid Syndrome, Protein C deficiency and Protein S deficiency , Antithrombin III deficiency and Factor V Leiden mutation .
꘎ Cancer
꘎ Collagen vascular disease like Lupus, Wegner's granulomatosis and Bechet syndrome
꘎ Obesity
꘎ Intracranial hypotension
꘎ Inflammatory bowel disease like Crohn's disease or Ulcerative colitis
Question3 : There was seizure free period in between but again sudden episode of GTC . Why? resolved spontaneously why ?
Answer: INTERICTAL PERIOD
- It refers to the period between seizures or convulsions that are characteristic of an epileptic disorders
- The interictal period correspond to more than 99 % of their life .
- The interictal period is often used by neurologist when diagnosing epilepsy since an EEG trace will often show small interictal spiking and other abnormalities known as subclinical seizures.
- Interictal EEG discharges are those abnormal waveforms not associated with seizure symptoms
Causes of Interictal period :
- The sodium gradient that allow the potential to be propagated is so large in comparision to tiny number of ion that are let through each channel with each signal that is highly unlikely that this gradient could be used up by high activity during a seizure .



Fig: Phases in GTCS
Question4. What drug was used in suspicion of cortical venous sinus thrombosis ?


Table : Difference between HFpEF and HFrEF

Fig : Heart Failure and Ejection Fraction

Fig. Comparison of HFpEF and HFrEF

Question2. Why haven't we done pericardiocentesis in this patient ?

Fig : Cardiac Tamponade and Pericardiocentosos



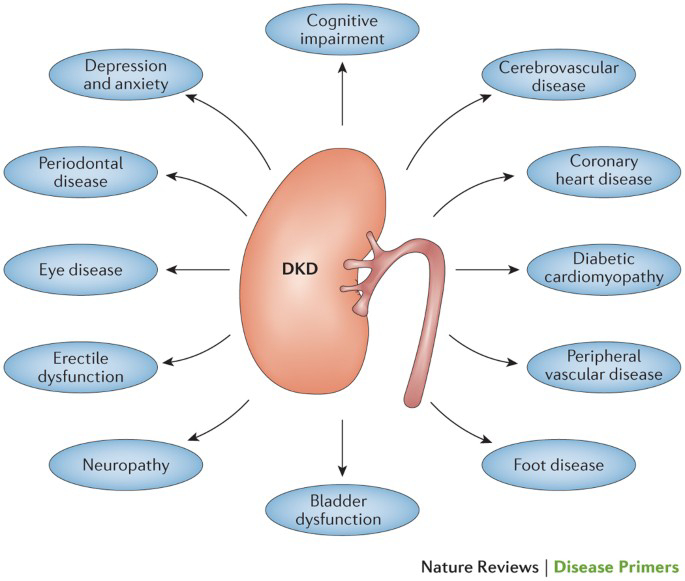
Fig : Complications of Long standing Diabetes

Table : Stages of CKD
- Mean baseline BP was 132/78 +/-9 mmHg - Following 4 weeks of treatment, changes in sitting BP were: Placebo = -1.9/-2.1 mmHg; ER metoprolol 0.2 mg/kg = -5.2/-3.1 mmHg; 1.0 mg/kg = -7.7/-4.9 mmHg; 2.0 mg/kg = -6.3/-7.5 mmHg. - Compared with placebo, ER metoprolol significantly reduced systolic blood pressure (SBP) at the 1.0 and 2.0 mg/kg dose (P = .027 and P = .049, respectively), reduced diastolic blood pressure (DBP) at the 2.0 mg/kg dose (P = .017), and showed a statistically significant dose response relationship for the placebo-corrected change in DBP from baseline. There were no serious adverse events or adverse events requiring study drug discontinuation among patients receiving active therapy.
Question1: What is the most probable diagnosis in this patient ?
Answer: The most probable diagnosis in this patient is Grade 3 RPD of right kidney .
. Differential diagnosis are :
Question 2. What was the cause of her death ?
Answer. The patient underwent Emergency Laparotomy in another hospital .
- May be due to the complications of Laparotomy the patient would have died .
- Complications of Laparotomy include:
Question3 : Does her NSAID abuse have anything to do with her condition ? How ?
Answer. NSAID induced Renal Dysfunction
- Adverse renal effects from these drugs are caused by two distinct pathological entities :

Fig :NSADs and Renal complications.
https://rishikoundinya.blogspot.com/2021/05/55years-old-patient-with-seizures.html
Question1. Is there any relationship between occurrence of seizure to brain stroke. If yes what is the mechanism behind it?
Answer . Seizures after ischemic strokes. - An increase in intracellular Ca2+ and Na+ with a resultant lower threshold for depolarization, glutamate excitotoxicity, hypoxia, metabolic dysfunction, global hypoperfusion, and hyperperfusion injury.
- Seizures after hemorrhagic strokes are thought to be attributable to irritation due to (hemosiderin deposits)caused by products of blood metabolism
- Late onset seizures are associated with the persistent changes in neuronal excitability and gliotic scarring is most probably the underlying cause.
2. In the previous episodes of seizures, patient didn't loose his consciousness but in the recent episode he lost his consciousness what might be the reason?
Answer. Initially the patient might have had Simple partial seizures (no loss of consciousness) and might have progressed to Generalised Tonic Clonic seizures (loss of consciousness).
https://nikhilasampathkumar.blogspot.com/2021/05/a-48-year-old-male-with-seizures-and.html?m=1
Question1. What could have been the reason for this patient to develop ataxia in the past 1 year?
Answer. The patient has minor unattended head injuries in the past 1 yr. According to the CT scan, the patient has cerebral hemorrhage in the frontal lobe causing probably for the occurrence of Frontal lobe ataxia .
2) What was the reason for his IC bleed? Does Alcoholism contribute to bleeding diatheses ?
Answer. The patient has minor unattended head injuries.
- During the course of time the minor hemorrhages if present should have been cured on their own.
- But the patient is a chronic alcoholic . This might have hindered the process of healing or might have stopped the healing rendering it to grow further more into 13 mm sized hemorrhages occupying Frontal Parietal and Temporal lobes .
http://shivanireddymedicalcasediscussion.blogspot.com/2021/05/a-30-yr-old-male-patient-with-weakness.html
Question1. The patient's history of road traffic accident have any role in his present condition?
Answer .The closeness of facial bones to the cranium would suggest that there are chances of cranial injuries. Since the Zygomatic arch and Mandibular process is very close to the cranium, this might play a role in the patient's present condition
Question2. What are warning signs of CVA?
Answer. Weakness or numbness of the face, arm or leg, usually on one side of the body
- Trouble speaking or understanding
- Problems with vision, such as dimness or loss of vision in one or both eyes.
- Dizziness or problems with balance or coordination.
- Problems with movement or walking
- Fainting or seizure
- Severe headaches with no known cause, especially if they happen suddenly
3.What is the drug rationale in CVA?
Answer.
Mannitol: Because of its osmotic effect, mannitol is assumed to decrease cerebral edema. Mannitol might improve cerebral perfusion by decreasing viscosity, and as a free-radical scavenger, it might act as a neuroprotectant.
Ecospirin: For the prevention of heart attack, stroke, heart conditions such as stable or unstable angina (chest pain) due to a blood clot.
Atrovas: Atorva 40 Tablet belongs to a group of medicines called statins. It is used to lower cholesterol and to reduce the risk of heart diseases. Cholesterol is a fatty substance that builds up in your blood vessels and causes narrowing, which may lead to a heart attack or stroke.
- Rt feed RT feed is a nursing procedure to provide nutrition to those people who are either unable to obtain nutrition by mouth or are not in a state to swallow the food safely.
4. Does alcohol has any role in his attack?
Answer. When the patient met with an accident there might be cranial damage which was unnoticed.
- If so his occasional drinking may or may not have hindered the process of the minor hemorrhages getting healed and might have caused this condition.
- But since the patient is not a chronic alcoholic and so Alcohol might not have played any role.
* Therefore it cannot be evaluated without further details
5.Does his lipid profile has any role for his attack??
Answer. The inverse relationship between serum HDL-C and stroke risk . When taken together it seems clear that higher baseline levels of serum HDL-C lower the risk of subsequent ischemic stroke.
https://kattekolasathwik.blogspot.com/2021/05/a-case-of-cardiogenic-shock.h
1. How did the patient get relieved from his shortness of breath after i.v fluids administration by rural medical practitioner?
Answer. Because of the fluid loss occurred to the patient
there is decreased preload- so, SOB occurred due to decreased CO
IV fluids administered- there is increased preload- SOB decreased due to better of cardiac output.
Question2. What is the rationale of using Torsemide in this patient?
Answer. Torsemide used to relieve abdominal distension.
3. Was the rationale for administration of ceftriaxone? Was it prophylactic or for the treatment of UTI?
Answer. IT IS THE TREATMENT FOR UTI
Rationale- Used for any bacterial infection.
https://drsaranyaroshni.blogspot.com/2021/05/an-eight-year-old-with-frequent.html
Questions1. Why is the child excessively hyperactive without much of social etiquettes ?
Answer. Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterized by inattention, or excessive activity and impulsivity, which are otherwise not appropriate for a person's age
- For a diagnosis, the symptoms have to be present for more than six months, and cause problems in at least two settings (such as school, home, work, or recreational activities).
Question2. Why doesn't the child have the excessive urge of urination at the night time ?
Answer. The child doesn’t have excessive urge of urination at night but at day there might be a psychiatry related condition
1. Psychosomatic disorder
2. Undiagnosed anxiety disorder
3. How would you want to manage the patient to relieve him of his symptoms ?
Answer. bacterial kidney infection, the typical course of treatment is antibiotic and painkiller therapy.
- If the cause is an overactive bladder, a medication known as an anticholinergic may be used. These prevent abnormal involuntary detrusor muscle contractions from occurring in the wall of the bladder
Question3. How do you want to manage the patient to relieve him of his symptoms ?
Answer. To treat attention deficit hyperactivity disorder:
** For children 6 years of age and older, the recommendations include medication and behavior therapy together — parent training in behavior management for children up to age 12 and other types of behavior therapy and training for adolescents. Schools can be part of the treatment as well.
- Methylphenidate: A stimulant and a medication used to treat Attention Deficit Hyperactivity Disorder. It can make you feel very ‘up’, awake, excited, alert and energized, but they can also make you feel agitated and aggressive. They may also stop you from feeling hungry.
- Amphetamine belongs to a class of drugs known as stimulants. It can help increase your ability to pay attention, stay focused on an activity, and control behavior problems .
https://preityarlagadda.blogspot.com/2021/05/biatrial-thrombus-in-52yr-old-male.html
Question1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Answer: the anatomical site is BLOOD VESSELS
* ETIOLOGY:
The physical stress of hypertension on the arterial wall also results in the aggravation and of atherosclerosis, particularly of the coronary and cerebral vessels. Moreover, hypertension appears to increase the susceptibility of the small and large arteries to atherosclerosis.
- The most likely cause of arterial thrombosis is artery damage due to atherosclerosis. Atherosclerosis occurs when a person has a buildup of plaque on the walls of their arteries. The arteries then begin to narrow and harden, which increases a person's risk of developing arterial thrombosis.
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Answer: PHARMACOLOGICAL INTERVENTIONS
1. TAB. Dytor
Mechanism: Through its action in antagonizing the effect of aldosterone, spironolactone inhibits the exchange of sodium for potassium in the distal renal tubule and helps to prevent potassium loss.
2. TAB. Acitrom
Mechanism: Acenocoumarol inhibits the action of an enzyme Vitamin K-epoxide reductase which is required for regeneration and maintaining levels of vitamin K required for blood clotting
3. TAB. Cardivas
Mechanism: Carvedilol works by blocking the action of certain natural substances in your body, such as epinephrine, on the heart and blood vessels. This effect lowers your heart rate, blood pressure, and strain on your heart. Carvedilol belongs to a class of drugs known as alpha and beta-blockers.
4. INJ. HAI S/C
Mechanism - Insulin and its analogues lower blood glucose by stimulating peripheral glucose uptake, especially by skeletal muscle and fat, and by inhibiting hepatic glucose production; insulin inhibits lipolysis and proteolysis and enhances protein synthesis; targets include skeletal muscle, liver, and adipose tissue
5.TAB. Digoxin
Mechanism: Digoxin has two principal mechanisms of action which are selectively employed depending on the indication:
- Positive Ionotropic: It increases the force of contraction of the heart by reversibly inhibiting the activity of the myocardial Na-K ATPase pump,
an enzyme that controls the movement of ions into the heart.
6. Hypoglycemia symptoms explained
7. Watch for any bleeding manifestations like Petechiae, Bleeding gums.
8. APTT and INR are ordered on a regular basis when a person is taking the anticoagulant drug warfarin to make sure that the drug is producing the desired effect.
Question 3: What is the pathogenesis of renal involvement due to heart failure (cardio-renal syndrome) . Which type of cardio renal syndrome is this patient ?
Answer: *cardiorenal syndrome type 4* is seen in this patient.
4) What are the risk factors for atherosclerosis in this patient?
Answer: Effect of hypertension
- They can also impair blood vessels' ability to relax and may stimulate the growth of smooth muscle cells inside arteries. All these changes can contribute to the artery-clogging process known as atherosclerosis.
5) Why was the patient asked to get those APTT, INR tests for review?
Answer: APTT and INR are ordered on a regular basis when a person is taking the anticoagulant drug warfarin to make sure that the drug is producing the desired effect.
- Here, an INR of 3-4.5 is recommended. Warfarin should be started in conjunction with heparin or low molecular weight heparin when the diagnosis of venous thromboembolism is confirmed, although local protocols may vary in their starting doses and titration schedule.
https://63konakanchihyndavi.blogspot.com/2021/05/case-discussion-on-liver-abcess.html
Question1: Cause of liver abscess in this patient ?
Answer: Cause of liver abscess in this patient is ENTAMOEBA HISTOLYTICA
Question2: How do you approach this patient ?
Answer: Approach in the patient of AMOEBIC LIVER ABSCESS
3) Why do we treat here ; both amoebic and pyogenic liver abscess ?
Answer: We treat the patient for both amoebic and pyogenic abscess so that we don't rely only on anti-amebic therapy and insure complete treatment of the cause
4) Is there a way to confirm the definitive diagnosis in this patient?
Answer : The confirmatory test for amoebic abscess is *Serologic testing* the most widely used method of diagnosis for amebic liver abscess.
- In general, the test result should be positive, even in cases when the result of the stool test is negative (only extra-intestinal disease).
- The diagnosis of amebic liver abscess was based on four or more of the following criteria:
(i) a space-occupying lesion in the liver diagnosed by ultrasonography and suggestive of abscess,
(ii) clinical symptoms (fever, pain in the right hypochondrium (often referred to the epigastrium), lower chest, back, or tip of the right shoulder),
(iii) enlarged and/or tender liver, usually without jaundice,
(iv) raised right dome of the diaphragm on chest radiograph, and
(v) improvement after treatment with antiamoebic drugs (e.g., metronidazole).

Comments
Post a Comment