Final Practical Long Case
Final practical
Arushi Kumari
roll.no-151
MBBS 9th semester
Appetite- decreased
Bowel and bladder- regular
Sleep- disturbed
Addictions- nil
Pallor +
no icterus
No cyanosis
No clubbing
no lymphadenopathy
No edema.
VITALS:
Patient was afebrile at the time of presentation .
BP: 110/70bmmHg ,B/L
PR: 72bpm , regular and normal volume,felt bilaterally
RR:18 cpm
SpO2 : 98 with RA
LOCAL EXAMINATION:
left lower limb swelling was present at ankle associated with redness and local rise of temperature and dorsalis pedis pulses were felt.
SYSTEMIC EXAMINATION
CVS
Inspection:
no scars on the chest
no features of raised JVP no additional visible pulsations seen
Palpation
all inspectory findings are confirmed
apex beat normal at 5th ics
no additional palpable pulsations or murmurs
percussion showed normal heart borders
auscultation S1 S2 heard no murmurs or additional sounds
CNS: C/C/C
MOTOR-: normal tone and power
reflexes: RT LT
BICEPS ++ ++
TRICEPS ++ ++
SUPINATOR ++ ++
KNEE ++ ++
SENSORY :
touch, pressure, vibration, and proprioception are normal in all limbs
GIT:
inspection- normal scaphoid abdomen with no pulsations and scars
palpation - inspectory findings are confirmed
no organomegaly, non tender and soft
percussion- normal resonant note present, liver border normal
auscultation-normal abdominal sounds heard, no bruit present
RESPIRATORY:
inspection: normal chest shape bilaterally symmetrical, mediastinum central
no scars, Rr normal, no pulsations
palpation: Inspectory findings are confirmed
percussion: normal resonant note present bilaterally
Related Images














Overall Investigations :
RBS: 136mg/dl
HEMOGRAM:
HB: 6.9
TC: 9700
MCV: 85.1
PCV: 21.7
MCH: 27.1
MCHC: 31.8
PLT: 1.57
ESR: 90
SMEAR: ANISOCYTOSIS
RFT:
Blood Urea: 20mg/dl
S. Creatinine: 1.1mg/dl
Na: 136
K: 3.3
Cl: 98
LFT:
TB: 0.45
DB: 0.17
AST: 60
ALT: 17
ALP: 138
TP: 6.3
ALB: 2.18
CUE:
ALB +
Sugars nil
Pus cells nil
ESR - 90
CRP - NEGETIVE
HCV: NEGETIVE
HBV: NEGETIVE
HIV: NEGETIVE

Fig : ANA report
Teeatment History
On 1st day ( 02/06/22 )
Inj. Piptaz 4.5 gm / iv / tid
Inj. Metrogyl 600 mL /iv / tid
Inj. Neonol 1 gm /iv / SOS ( if temp more than 101 F )
Tab. Chymoral forte PO/ TID
Tab Pan 40/ PO/ OD
Tab teczime 10 mg / PO/ OD
Hydrocortisone cream 1 per cent / OD face * week
Tab Orofer XT / OD
Inj. Nervz 1 amp in 100 mL NS
On day 2 ( 03/08/22 )
Inj. Piptaz 4.5 gm / iv / tid
Inj. Metrogyl 600 mL /iv / tid
Inj. Neonol 1 gm /iv / SOS ( if temp more than 101 F )
Tab. Chymoral forte PO/ TID
Tab Pan 40/ PO/ OD
Tab teczime 10 mg / PO/ OD
Hydrocortisone cream 1 per cent / OD face * week
Tab Orofer XT / OD
Inj. Nervz 1 amp in 100 mL NS
On day 5 (06/06/22 )
Tab Deflezacort 6mg / PO /BD
Tab Cefixime 200 mg / PO / BD
Tab. Orofer XT / PO / OD
Tab. Teczine 100 mg / PO/OD
Tab Rantac 150 mg / PO/OD
Hydrocortisonebcream 1 per cent OD for face * 1 week
Onlast day ( 07/07/22 )
Tab Deflezacort 6mg / PO /BD
Tab Cefixime 200 mg / PO / BD
Tab. Orofer XT / PO / OD
Tab. Teczine 100 mg / PO/OD
Tab Rantac 150 mg / PO/OD
Hydrocortisonebcream 1 per cent OD for face * 1 week
PROVISIONAL DIAGNOSIS:
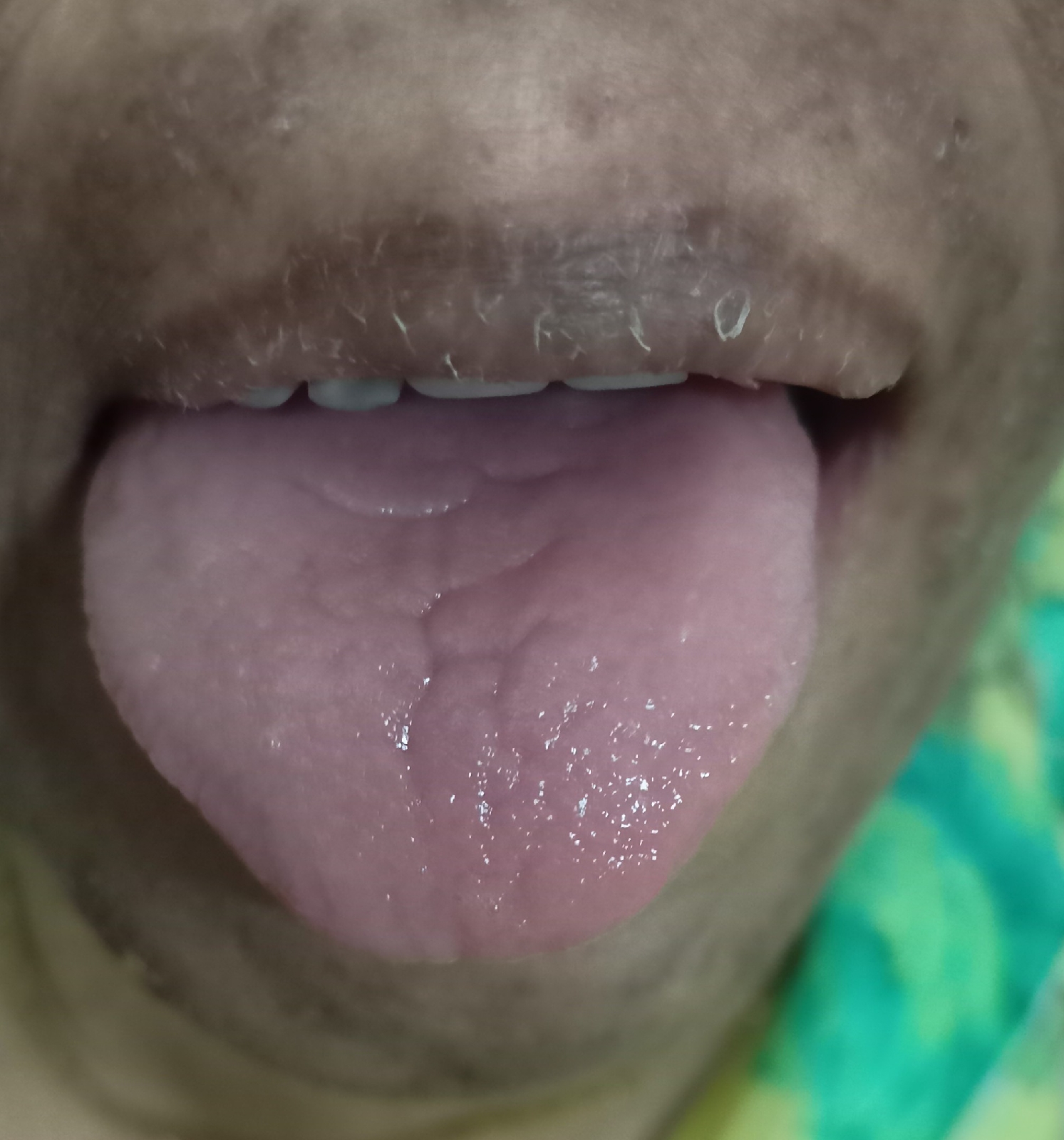
? Secondary sjogren syndrome
Anaemia secondary to chronic inflammatory disease
with Left Lower limb cellulitis
B/L Optic atrophy

Comments
Post a Comment