GENERAL MEDICINE E - LOG BOOK
1st December 2021
 Done on 01/12/21
Done on 01/12/21
 Done on 01/12/21
Done on 01/12/21
 Done on 01/12/21
Done on 01/12/21
 Done on 01/11/21 ( at 7:04 a.m )
Done on 01/11/21 ( at 7:04 a.m )
 Done on 01/12/21
Done on 01/12/21



 MRI Report
MRI Report


This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment .
ARUSHI KUMARI
Roll no. 151
60 YEAR OLD MALE WITH ACUTE ON CHRONIC SUBDURAL HEMATOMA
A 60 year old male , farmer by occupation presented to the OPD on 30th November with chief complain of recurrent episodes of vomiting and giddiness .
History of Presenting Illness
- Patient was apparently asymptomatic 15 days ago then he started to vomit after every meal preceded headache , mild giddiness and heat sensation on his forehead .
- Patient complaint of giddiness follwed by vomiting for 10-15 mins .
Past History
- History of trauma on scalp 4 month back following by swelling and bleeding .
- bleeding stopped within sometime after applying icepack .
- History of fight 2 months ago due to which he got injury on left temporal region. He visited RMP and doctor prescribed antihypertensives which he took for 2 days and then stopped ( as said by patient )
- History of repeated vomiting from 15 days because of which patient became very weak and was not able to walk .
- So the relative themselves kept a catheter 15 days back for convenience as he had repeated vomiting and was not able to walk .
- Not a known case of Asthma, HTN , epilepsy , diabetes , thyroid , TB .
PERSONAL HISTORY
- Appetite normal
- Mixed diet
- Sleep is adequate
- Bowel and bladder movements are normal
- history of allergic reaction on upper gluteal region 20 days back which subsided within 4-5 days by applying ointment by local doctor
- Same episode of allergic reaction since 1 year ( 4 times in last 1 year )
- Chronic smoker from last 40 years ( stopped since 15 days )
GENERAL EXAMINATION
Patient was examined in well lit room with his consent .
Patient is conscious ,coherent and cooperative
Patient is well oriented to time and place
Moderately built and nourished
Pallor:absent
Icterus: absent
Clubbing:absent
Cyanosis:absent
Lymphadenopathy: absent
Edema: absent
VITALS
Temperature: afebrile
Pulse: 60 / min
Respiratory rate : 18 bpm
Blood pressure : 160/100
SpO2 at room air : 98 per cent
GRBS : 147 mg/dL
SYSTEMIC EXAMINATION
Cardiovascular system
s1 and s2 heard ,no murmurs
Respiratory system
Central position of trachea
Vesicular breath sounds
No wheeze,no dyspnea
Abdominal examination
Scaphoid shape
No tenderness
No palpable masses
No bowel sounds
CNS EXAMINATION
HMF : intact
Cranial nerve : intact
R L
- Vibration
- Wrist PRESENT PRESENT
- Elbow PRESENT PRESENT
- LL PRESENT PRESENT
- Proprioception P P
Motor system:-
Tone :
R L
Upper limbs: N N
Lower limbs: N N
Power:-
R L
Upper limbs: 4+ 4+
Lower limbs: 4+ 4+
Reflexes:
B T S K A
Right - 3+ 3+ 3+ 3+ 3+
Left - 3+ 3+ 3+ 3+ 3+
Plantar - Flexors
INVESTIGATION :
On 01/12/21 at 7:00 a.m
CBP :
Hb - 9.9
TLC - 5,600
PLT - 1.96 L
CBP at 1:00 a.m
Hb - 10.4
TLC - 6,600
PLT - 2.11 L
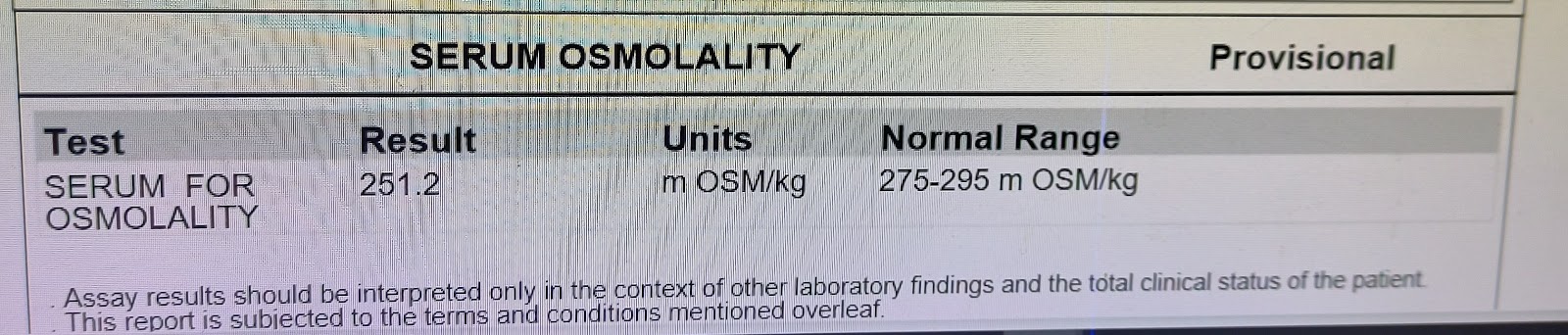
Serum electrolytes
Na+ - 148
K+ - 3.5
Cl - 95
CUE
Albumin - ++
FBS - 95mg/dL
Serum Creatinine - 1.0 mg/dL
Blood urea - 39 mg/dL
OPHTHALMOLOGY REFERRAL
( 01/12/21 )
R L
Lids N N
Conjunctiva quiet quiet
Cornea clear clear
Pupil drug drug
mydriasis mydriasis
Lens Early Lo Early Lo
Dilated Funds Examination
R L
gross tessellation + gross tessellation +
Disc N disc , circular blurring of nasal margins
well defined pale disc
margins N site , circular
CDR 0.3-0.4 : 1
Vessels N N
Macula FR dull not seen
Impression : No features of raised ICT noted .


CLINICAL PICTURE


Provisional Diagnosis : Acute on chronic subdural hematoma
TREATMENT :
DAY 1 :
- INJ OPTINEURON 1 Amp in 100ml NS/IV/OD
- INJ ZOFER 4mg IV/TID
- Tab PAN 40mg OD
- Tab ONDANSETRON CHEWABLE TABLETS TID
- BP/ PR/ Temperature monitoring every 4th hourly
- Dextrose Saline 2 unit
- 100 mL Normal saline
DAY 2 :
Inj. OPTINEURON 1 amp in 100 mL IV/ID
Inj. ZOFER 4 mg IV/ TID
Tab PAN 40 mg OD
BP : 120/70 mmHg
PR : 62

Comments
Post a Comment